Extract, place, restore. One visit.
Traditional implant treatment for a failing front tooth involves three separate stages: extraction (with months of healing), implant placement (with months more healing), and finally the crown. The patient lives without a visible front tooth — or with an awkward removable flipper — for most of a year.
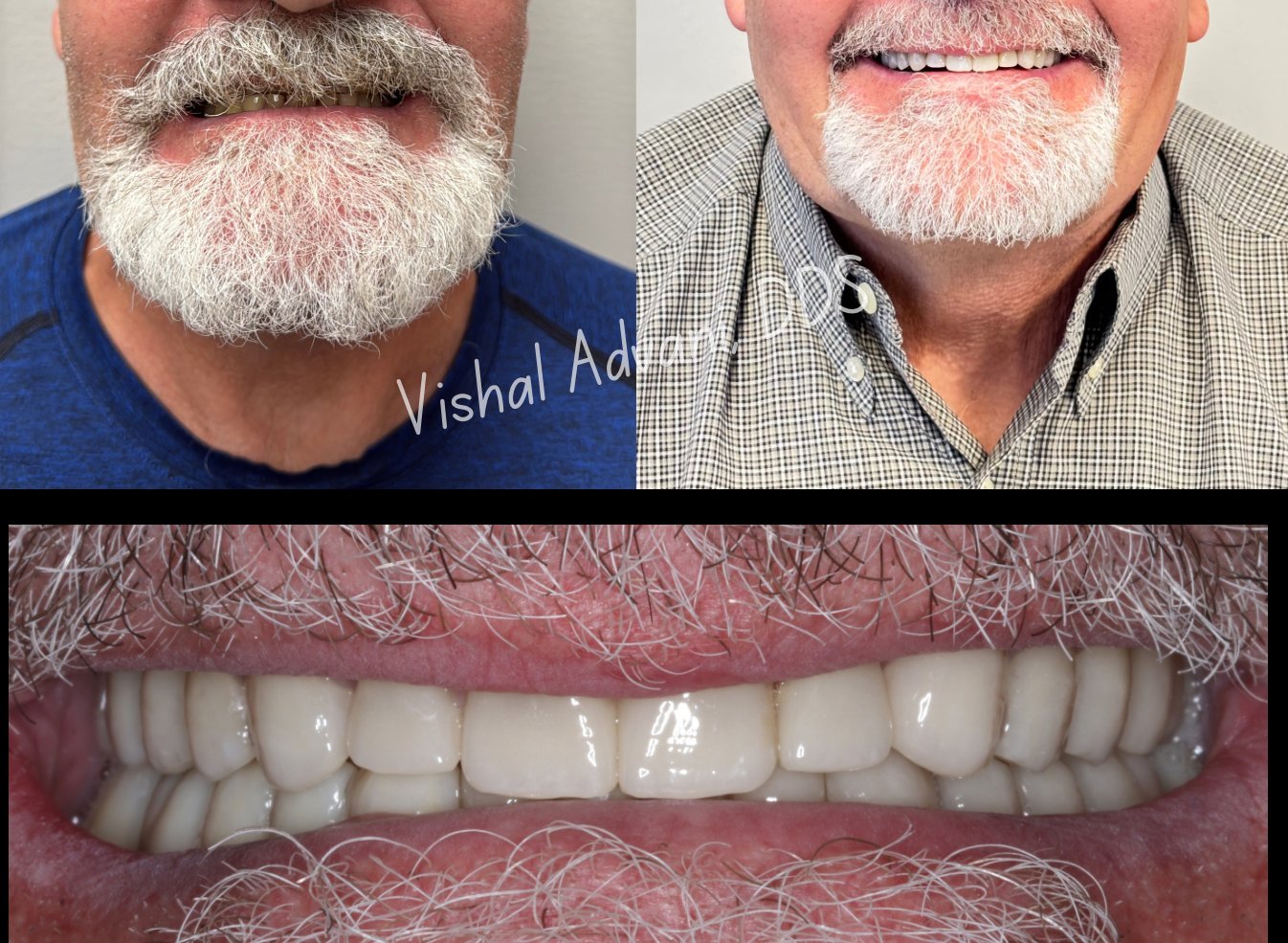
Anterior immediate placement compresses this to a single surgical visit. The failing tooth is extracted, the implant is placed in the same socket, and a custom-shaped temporary crown is delivered the same day. You leave with a complete smile that looks indistinguishable from your natural teeth — even though osseointegration is still occurring beneath the surface.
The technique is demanding. The buccal bone in the anterior maxilla is naturally thin, the gum biotype is often delicate, and the aesthetic margin for error is essentially zero. This is exactly why we use X-Nav dynamic navigation for these cases — sub-millimeter precision is the difference between a result that looks natural and one that looks like an implant.
