What is FP1 surgery?
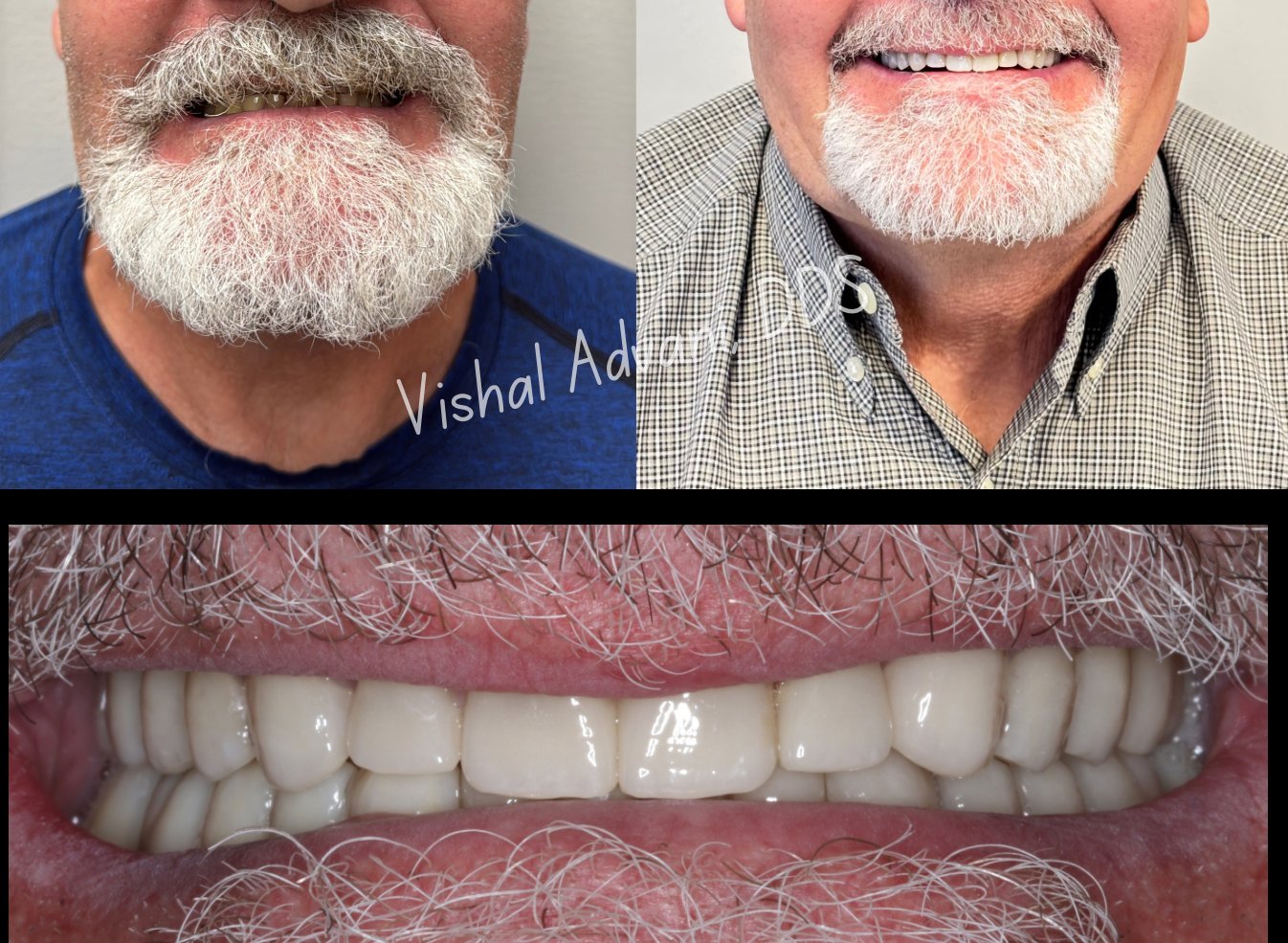
The "FP1" classification — short for Fixed Prosthesis Type 1 — describes a dental implant restoration that replaces only the crown of the missing tooth, with the gum line and surrounding tissue preserved exactly as nature created them. The result is an implant that looks indistinguishable from a real tooth, even when smiling fully.
The challenge is that FP1 only works when the bone and soft tissue around the extraction site are preserved. The moment a tooth is removed, the body begins reabsorbing the bone and gum that supported it — and within months, what remains is often inadequate for a true FP1 result. This is why most implant cases default to FP3, where pink prosthetic gum material is added to compensate for lost tissue.
FP1 surgery uses biological preservation techniques at the time of extraction to keep the tissue architecture intact — so when the final crown is placed, the result is a natural smile, not a prosthetic one.
